The Burrow
Jun 8, 2021
Humans have always been fascinated by artificial objects. From ancient Egyptian toys and marble Renaissance sculptures to modern sci-fi films and AI technology, we’ve been re-imagining our artificial creations over and over.
As such, it’s no wonder we’re sharing an increasingly intimate space with our technological fascinations; so much so that some of us rely on them to live and maintain our quality of life in the face of illness.
For many, that comes in the way of life-saving medical devices. From cochlear implants to pacemakers, there are a range of devices that have been specially created to keep us alive. Also known as medical human information and communication technology (ICT) implants, they are a very important part of our way of life. Medical human ICT implants are therapeutic devices placed inside or on the surface of the body, which may deliver medication, monitor body functions or provide support to organs and tissues.1,2
Lucky for some, if a specific medical device is medically necessary, you may be able to claim the costs of the device through a private health insurance policy, depending on a few factors, including your level of cover, what’s included in your policy, and whether your device is deemed medically necessary.
If you require an ICT implant and are interested in recuperating some costs through a health policy, we suggest speaking with your fund to see what requirements need to be met. Or, if you are looking to get cover for the first time, speak with the health insurance experts at Compare the Market to see what options you have across a variety of funds.
Given our interest in the health and wellbeing of Australians, we’ve decided to explore the merge of man and machine by delving into the history of medical implants. Read on to discover some of the amazing devices that have been invented throughout history!
We’ve selected medical human ICT implants that are or were commercially available. These implants are or were typically implanted inside or partially inside the human body. We’ve excluded prosthetics, birth control implants, developing implantable nanotechnology, cosmetic implants and dental implants.
The cochlear implant (CI) was the first effective treatment for deafness and severe hearing loss. It takes between six months and a year for the sound quality to improve, but the implant lasts a lifetime. There are four CI manufacturers:
1. Cochlear Limited (Australia),
2. MedEl Corporation (Austria),
3. Advanced Bionics (USA, a division of Sonova) and
4. Neurelec (France, a division of William Demant).3
N.B. Only the first three are FDA-approved for use in the United States.
Neurelec is used in Europe, Asia, Africa, South America and Canada. In recent times, a fifth manufacturer, Nurotron from China, has become available in some parts of the world.3 In Romania, the models available include Cochlear Limited, MedEl Corporation and Advanced Bionics.3
When you get a cochlear implant fitted, you’ll receive general anaesthesia so that you’re comfortable during the two-to-three hour procedure. The surgeon will make a small incision behind your ear before threading the electrodes into your cochlea.4 After the initial procedure, an audiologist will help adjust the device over several sessions while you rehabilitate your brain to recognise and interpret sounds.
The device is meant to last a lifetime, but if it needs to be replaced due to equipment failure, advancing technology or other reasons, a surgeon could remove and replace it for you.4
1800 – Alessandro Volta uses an electric current to stimulate the inner ear.3
1957 – In Algeria, André Djourno (medical physicist) and Charles Eyriès (otologist) performed the first direct electrical stimulation of the human auditory system.3
After implanting an electrode and induction coil into the temporal muscle, a patient was able to differentiate various sound intensities. However, patients couldn’t understand speech or differentiate speech among various speakers. The device failed after a few weeks and was therefore discontinued.
1961 – Dr House (otologist) and Dr John Doyl (neurosurgeon) created the first cochlear implants, which helped patients notice the audible changes in sound, including loudness and pitch. This development took 10 years and was first implanted in a patient in 1972. The device continued to be used until 1985.3
1971 – The single-channel device (one electrode that stimulates nerve fibres in the ear) was developed in the US. Graeme Clarke and his team in Australia investigated the limitations of single-channel devices and realize the need for a multi-channel device (multiple electrodes that stimulate various nerve fibres).3
1973 – Clarke partnered with physician David Dewhurst to develop a cochlear implant prototype, which they called the bionic ear.
1975 – In Austria, ear, nose and throat (ENT) professor Kurt Burian applied for a €10,000EUR research grant from the Austrian research council, which he used to launch a single then a multi-channel device.3
1978 – After looking for deaf recipients for two years, Clarke and his team implanted an Australian multi-channel CI into a patient for the first time. At this point, Clarke and his team had developed a smaller and more portable speech processor. The Australian team partnered with Nucleus to market their new bionic ear.3
1982 – Burian’s pupil Ingeborg Hochmair and her husband Erwin launched the MedEl implants in Austria.3
1984 – In Australia, the Cochlear Company – founded by Graeme Clark (ENT) – introduced the first multi-channel cochlear implant system.3
1985 – Clarke’s research determined that the Nucleus multi-channel device was more effective than their single-channel devices. The FDA also approved the Nucleus device to treat post-lingually deaf patients (people who became deaf after learning speech and language).3
1986 – Clarke founded the Bionics Institute – an institute that helps develop technologies for eyes, ears and the central nervous system.
1995 – Australian Stock Exchange lists Cochlear Limited as a separate company.3
1996 – The FDA approves Advanced Bionics Company’s multi-channel Clarion cochlear implant.3
1997 – The FDA approves the Clarion cochlear implant for use in children.3
2001 – The development of the CII Bionic Ear implant and HiFocus electrode allowed software updates to be programmed into the device to minimise surgery frequency.3
2002 – The T-Mic™ microphone allowed recipients to connect their implants to their phones, headsets and MP3 players.3
2003 – Advanced Bionics developed the HiRes 90k implant.3
2006 – Advanced Bionics developed the Harmony CI.3
2011 – The Bionic Ear Institute changed its name to Bionics Institute.
2020 – Today, cochlear implants are battery-powered sound processors that look like hearing aids. They’re worn behind the ear where a small microphone can capture sounds and send signals towards the inner ear.4
An implantable cardioverter defibrillator (ICD) is a battery-operated device that corrects abnormally fast heart rhythms by administering a small electric shock.10 If you’re an eligible candidate for this device, you’ll receive local anaesthesia to help you relax before surgery. Some people are sedated with general anaesthetic.11
The pulse generator part of the ICD usually needs to be replaced every 5-15 years. A surgeon will make a small incision to disconnect the generator from the leads before replacing it. Leads normally don’t need to be replaced, but if they get damaged, a more complex surgery may be required to remove them.12
1969 – In the US, Michel Mirowski and Morton Mower created the first prototype for the ICD.5
1970 – Mirowski and Mower gained major support to develop the ICD, but they decided there was no market for it.5
1972 – Mirowski met Stephen Heilman, owner of a small medical company called Medrad. Heilman provided Mirowski and Mower with a team of medical engineers to continue developing the ICD.5
1975 – Mirowski and Mower created a prototype small enough to implant into a dog. Film footage of the dog being defibrillated to life put the ICD at the forefront of cardiac research.5
During the 80s, the device was designed to treat ventricular fibrillation (rapid and erratic heart rhythm that causes the heart to quiver instead of pumping blood) with a high-energy shock. However, the device couldn’t detect ventricular tachycardia (a fast, abnormal heart rate), which could progress to ventricular fibrillation.
The devices couldn’t be programmed before the 90s, which meant that secondary pacemakers had to be used for bradycardia pacing (slow heart rates).6
1980 – After further developments, the ICD was implanted into a person for the first time. However, its weight was 225g, it was only capable of defibrillation and it required a thoracotomy (surgical incision into the chest).
1985 – The first ICD was approved by the United States Food and Drug Administration (FDA). The implant required electrodes to sit directly on the surface of a heart. Surgeons also needed to implant the device into the wall of the upper abdomen because it was too big to sit inside the chest.
1990s – The device was developed to be wired through a vein that reached the inside surface of the heart, which decreased the recovery time and made the implantation procedure much easier.
Developers further refined the ICD to reduce its weight and size, and to feature full pacemaker abilities. The device was also able to perform a synchronised cardioversion for ventricular tachycardia (fast, abnormal heart rate).5
1991 – The Clinical Applications and Prevention Advisory Committee approved an antiarrhythmic versus implantable defibrillator (AVID) study. The AVID study compared treatment of antiarrhythmic drugs to implantable cardioverter-defibrillators in patients with life-threatening ventricular arrhythmias (VA). Ventricular arrhythmias are abnormally fast heartbeats in the lower chambers of the heart (ventricles).
1996 – A Multicenter Automatic Defibrillator Implantation Trial (MADIT) was conducted to test whether prophylactic therapy (preventative/suppression therapy) with an ICD, as opposed to pharmacotherapy (therapy with pharmaceutical drugs), would improve the survival rate of patients at high risk of VA. The study found that ICDs reduced the total mortality rate by 54 per cent.9
1997 – The AVID study was stopped early because it found that after one year, there was a 38 per cent reduction in deaths in people who had the implant compared to those taking the antiarrhythmic drug. The group who had the implants also saw a 25 per cent reduction in deaths in the second and third year of the experiment.7
2002 – A MADITII was conducted to evaluate the prophylactic benefit of ICD placement in patients with coronary artery disease and a left ventricular ejection fraction (the amount of blood pumped out by the left ventricle with each contraction) of less than 30 per cent – 55 per cent is considered normal. Patients who’ve previously had at least one heart attack, but required no further risk assessments, were picked for the trials. During the 20-month follow-up examination, mortality rates were 28 per cent lower for those in the ICD group.8
A dual chamber and VVI Implantable defibrillator (DAVID) trial is conducted to treat left ventricular dysfunction with optimized drug therapy and by pacing both left and right chambers of the heart. The goal of this trial was to improve the mortality and heart failure hospitalisation rates.8
DAVID trials were stopped early (2002) because dual-chamber pacing offered no clinical advantage, and it may have been detrimental – the trials observed an increased death and hospitalisation rate.8
Modern models are also capable of performing anti-tachycardia pacing (anti-overdrive pacing) to stop ventricular tachycardia without sending electrical shocks to the patient’s heart. Some ICDs are also able to provide cardiac resynchronisation therapy (biventricular pacing); this is where a device is used to synchronise the rhythm of both sides of the heart for patients with advanced heart failure.5
2020 – Today, ICDs help detect and correct abnormal heart rhythms. The device is just smaller than a deck of cards and is normally inserted under the skin of your upper chest.
Bionic eyes deliver artificial vision through microelectrodes. These microelectrodes stimulate the optic nerves by sending electric pulses from the eye to the brain.11 This activity stimulates the parts of the visual system that isn’t functioning correctly.13 Currently, only those with degenerative retinal diseases can get bionic eyes.13
Australia and the United States are currently at the forefront of bionic eye development.
Early 1990s –Mark S. Humayun, Eugene de Juan, Gislin Dagnelie, et al experimented with electrical stimulation of the retina with the support of the Foundation for Fighting Blindness.13
1998 – Humayun et al developed a long-term implantable device that could restore vision in people with retinitis pigmentosa (breakdown of cells in the retina).8 During this time, Sam Williams and Alfred Mann founded Second Sight Medical Products with Robert Greenberg, Aaron Mendelsohn and Gunnar Bjorg.14
2002 – In the US, Humayun implanted the first Argus I in a patient as part of a clinical trial.14
2005 – In Germany, Retina Implant AG’s manufactured the Alpha IMS device to restore vision in patients with retinitis pigmentosa. The device offers treatment for patients who are completely blind.
2007 – In a series of clinical trials, doctors from Second Sight Medical Products implanted the first Argus II in the US.15, 14 The Argus II was designed to be smaller and easier to implant.
2009 – Professor Paulo Stanga conducted the first clinical trials for Argus II in patients with retinitis pigmentosa (RP) in the UK.16 The FDA approved the use of Argus I to treat fewer than 4,000 individuals per year.
The Argus II converts images from a video camera to a high contrast representation, which is further processed through electrodes to deliver vision to the eye. Recipients are able to see bright flashes arranged to represent basic shapes and approximate location of objects.17
2011 – The European Union approved the Argus II with a CE mark, a mark that indicates a product has passed the safety, health and environmental requirements and therefore is marketable in Europe.18 This model also became commercially available in Italy.15
2012-2014 – Bionics Institute conducted clinical trials for their novel suprachoroidal (between the sclera and choroid of the eye) retinal prosthesis in Australia, which would provide a better degree of surgical safety for patients.19,20 Three patients were implanted with this prosthesis with great results, but use was restricted to the lab. The prosthesis allowed patients to navigate outside and without supervision inside the home.
2013 – An external camera was fitted into the Bionics Institute’s bionic eye, allowing patients to identify basic letters, numbers and shapes.
The FDA approved the Argus II in the US.15
The Alpha IMS device gained a CE mark of approval.17
2014 – Bionic’s Institute’s bionic eye became more portable and allowed users to move around defined obstacles (within a laboratory setting.
In the US, the first commercially available Argus II was implanted.15
2015 – Health Canada approved the Argus II. Bionic eyes were implanted into a patient with age-related macular degeneration (a disease causing vision loss) for the first time in the UK.15
2018 – Australian company Bionic Vision Technologies Ltd ran clinical trials for a two-year pilot study on the BVT Gen2 suprachoroidal retinal prosthesis.20,21
2020 – Bionic Vision Technologies Ltd reported significant improvement in both obstacle awareness and detection. At 44 weeks, patients could detect up to 74.3 per cent of obstacles with the device, compared to 4% without the device.22
There is currently limited public information on the implant procedure and replacements for bionic eyes.22
Phakic intraocular lenses (IOL) are contact lenses that can be permanently implanted into the eye primarily for the treatment of myopia, which eliminates the need for optical aids (i.e., glasses or reusable contacts).27 There are three types of phakic IOL implants:
1. angle-supported (anterior chamber)
2. iris-fixated (anterior chamber)
3. posterior chamber.24
Angle-supported implants are lenses that are implanted between the iris and cornea, whereas posterior chamber implants are lenses that are implanted between the iris and lens (deeper in the eye). The difference between angle-supported and iris-fixated implants is where the angle is fixated. The first kind fixates itself between the space between the iris and cornea (iridocorneal angle), whereas the second fixates itself on the iris.
Intraocular lenses are different from phakic intraocular lenses; these replace the eye’s natural lens entirely, whereas phakic IOL implants do not.24 IOL implants are used to replace the eyes’ natural lens after cataract surgery (removal of the eyes’ cloudy natural lens) or aphakia.24 The phakic IOL lenses initially caused serious complications, but with further developments and modifications, the rate of complications has significantly decreased.24
The entire procedure normally takes around 20-30 minutes, but this may vary depending on your surgeon.28 The lenses are meant to last a lifetime, but they can be replaced or removed with surgery if needed. Phakic IOL lenses are suitable for patients who have a stable prescription. There may be other criteria that will determine whether you’re a suitable candidate for these implants. To find out more, consult your local ophthalmologist or optometrist.27
1953 – In Italy, Dr Strampelli (surgeon) created the Strampelli IOL to treat myopia (short-sightedness) and aphakia (absence of eye lenses). This IOL was placed in the eye’s anterior chamber, which sits between the iris and cornea. Strampelli’s IOL would later be the building block for many IOL developments.23
1984 – Iris fixated lenses were introduced by Jan Worst.24
1986 – Angle-supported phakic intraocular lenses (pIOLs) were first implanted. In Russia, posterior chamber IOLs were invented by Fyodorov, and they became available in two models: the implantable contact lens and the phakic refractive lens.25
1999 – Tobias H. Neuhann, MD, was the first surgeon to implant the Toric intraocular lens (TICL).26
2003 – In Switzerland, the Visian Implantable Collamer Lens (ICL) became internationally available.24 TICL received a CE mark in Europe – a mark that indicates a product has passed the safety, health and environmental requirements and therefore is marketable in Europe.18
2004 – The FDA approved the polymethyl methacrylate (PMMA) model (iris-fixated).24
2005 – The FDA approved use of Visian Implantable Collamer Lens for myopia between 3.00 and 20.00 diopters (a unit reciprocal to of focal length).24 These are the most widely implanted lens today.24
TICL was approved for use in Canada.
2007 – All designs for angle-supported that were commercially available were withdrawn due to high risks of endothelial decompensation (when the cells of the cornea break down) and other complications.24
2020 – Today, phakic intraocular lenses are used to treat myopia (short-sightedness) and hyperopia (long-sightedness). The lenses are about the size of a contact lens and they can be inserted through an incision placed just in front or behind the iris.27
IOL implants can used to replace the eye’s natural lens for patients who have cataracts. ICL can be used as a secondary lens to further improve your vision.27
Pacemakers are implantable devices that administer small electrical pulses to regulate abnormal heart rhythms.30 Pacemakers used to be an expensive service with charging systems too complicated for the elderly.29 Several issues delayed the widespread use of the original implantable pacemakers, including:
• faulty batteries
• bodily fluids leaking into the encasement
• broken leads.29
Before the procedure, your doctor may ask you to fast and take a blood sample to check how long your blood takes to clot. Your doctor may also administer blood-thinning medication a few days before the operation.29 During the procedure, a surgeon will administer local anaesthetic before making a small incision under the collarbone to insert the pacemaker. They’ll thread the leads through your blood vessels and into your heart. The entire procedure usually takes 1-2 hours, but it may take longer depending on your medical history. 29,30
Like the implantable cardioverter defibrillator (ICD), you may need to replace the pulse generator every 5-15 years. To replace the device, your doctor will administer local anaesthetic to remove the old device before replacing it with a new one. The pulse generator is about the same size, if not smaller, as a deck of cards.30
1932 – In the US, Albert Hyman (physiologist) created the ‘artificial pacemaker’ – a unit that sat externally from the body. This unit generated electrical pulses into a patient’s right atrium (one of the heart’s four chambers). Pulses could be delivered at 30, 60 or 120 beats per minute.29
1949 – John Hopps developed the first electronic cardiac pacemaker (external unit).29
1951 – Paul Zoll, a Boston cardiologist, developed an external tabletop pacemaker (electrodyne PM-65 pacemaker) that helped treat heart block . While it was effective, it was far too strong for young children.29
1956 – Aubrey Leatham and Geoffrey Davies developed an external stimulator, which helped resuscitate patients.29
1957 – Earl E Bakken (electrical engineer, TV repairment and co-founder of Medtronic Inc.) developed the first battery-operated wearable pacemaker. Infection frequently occurred along the wire of the partially implanted pacemaker. Most patients kept it on for a few weeks, but one kept it on for 15 months.29
Recurring heart blocks in these patients, who had recovered with the pacemaker, caused several deaths, and it became apparent that a pacemaker that could be used indefinitely was needed.29
1958 – In Sweden, Ake Senning (surgeon) and Rune Elmqvist (physician) invented the first implantable pacemaker.29
1958 – Wilson Greatbatch (electrical engineer) accidentally found a way to create an implantable pacemaker, which he patented in 1959. He took it to Dr William Chardack and Dr Andrew Gage, who helped test the viability of the product.29
1960 – Greatbatch later invented the long-life corrosion-free lithium-iodine battery to power the pacemaker.29
1961 – Zoll and Kantrowitz et al. successfully developed other pacemaker models.29
Mid-60s – Pacemakers could be implanted without a thoracotomy and without general anaesthesia.29
1970s – The lithium-iodine battery provided better longevity for the pacemaker, and therefore replaced the formerly popular mercury oxide-zinc battery.29
1972 – Parsonnet et al. invented the American-made nuclear radioscope pacemaker. This pacemaker had a lifespan of 20 years, but the extensive regulatory paperwork required to implant this made it unpopular.29
1980s – Pacemakers were made to respond to the heart’s activity level. Patients could adjust the pulse rate as needed.29
1990s – Microprocessors appeared on the market, which allowed the pacemakers to automatically modify the internal pacing parameters, depending on the patient’s needs.29
2000s – Biventricular heart pacing was introduced – an effective measure for heart failure. This is where a device is used to synchronise the rhythm of both sides of the heart for patients with advanced heart failure.29
2020 – Today, pacemakers are used to monitor and regulate abnormal heart rhythms. They’re just smaller than a deck of cards and will usually be inserted under the skin in the chest wall.
A spinal cord stimulator (SCS) is a device that administers electrical pulses through the spine to stimulate nerve activity, which curtails pain sensations from reaching the brain.31 It’s used to treat medical conditions that may cause pain, such as hypertension, angina, peripheral disease, back pain, and others.
A pulse generator with a non-rechargeable battery needs to be surgically replaced every two to five years, whereas a rechargeable battery may last eight to 10 years. To replace the battery, your surgeon will perform a simple surgical procedure.32 Rechargeable batteries may need to be recharged daily.33
1967 – Spinal cord stimulation (SCS) is used for the first time in the US. Invented by Norman Shealy (neurosurgeon), SCS was a modification of Barostat (used to treat hypertension) and Angiostat (used to treat angina – chest pain caused by restricted blood flow).31
1968 – SCS became commercially available through Medtronic in the US.31
1971 – SCS is used for the treatment of torticollis (neck muscle contraction) by Gildenberg.31
1976 – Cook and Dooley discover that SCS improves spasms. Dooley also discovers that SCS improves blood flow.31
1985 – Augustinsson et al. treated peripheral vascular disease (narrowing blood vessels) with SCS.
1987 – Murphy and Giles treat angina with SCS.31
1989 – the FDA approves the use of SCS to treat back pain and avoid back surgery.31
2020 – Today, candidates for SCS are required to trial the device to determine whether this implant is a suitable and effective long-term treatment for their condition. Once their suitability is determined, the device will be implanted and programmed to treat your condition.32
The SCS device is about the size of a pacemaker (a deck of cards) and it’s designed to last several years (as long as the battery lasts).
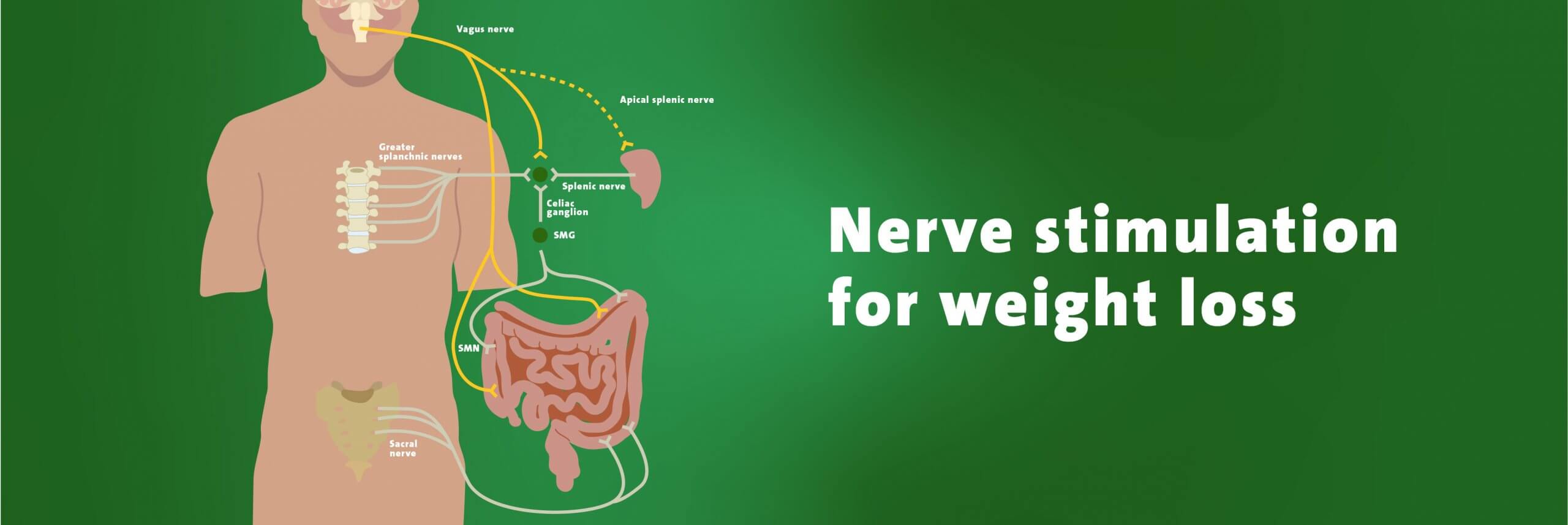
Leptos Biomedical is a company that offers neuromodulation therapy services for chronic obesity.34 Neuromodulation involves stimulating the splanchnic nerve. The splanchnic nerve carries neurons to the hypothalamus (a region in the brain), which supplies nerve activity to various organs involved with digestion, heart rate, blood pressure, satiety, feeding and weight gain.34 Theoretically, stimulating this nerve should result in reduced food intake and increased energy expenditure.34
To stimulate this nerve, a wireless electrode is inserted via a needle into the patient’s back, close to the splanchnic nerve. This electrode receives radiofrequency signals to stimulate the splanchnic nerve.34
Vagus nerve stimulation can also be used to help with weight loss or to treat epilepsy by reducing the frequency and intensity of seizures. The Maestro system, a pacemaker-like device, helps patients lose weight by blocking hunger signals from the vagus nerve. Blocking the vagus nerve results in:
• reduced food (caloric) intake
• increased feelings of satiety by delaying food processing.35
This device is implanted in the chest and the leads are attached to the vagus nerve in the patient’s neck.36
2002 – Leptos Biomedical is founded by Dr John D Dobak.34
2010 – Leptos Biomedical announced its closure. Reasons not provided.34
2002 – Enteromedics was founded.34
2011– Enteromedics’s Maestro Rechargeable System received the CE mark for obesity treatment and approval from the TGA.35
A study on seizures found that a third of people experienced at least a 50% reduction in seizures with vagus nerve stimulation. A third of people also experienced a 30-50% reduction in seizures.36
A quarter of people didn’t feel any positive effects at all, while less than 5% became seizure free.36
2015 – The FDA approved the Maestro Rechargeable System.37
2017 – European patent certificate for the Maestro system in Europe.38
2020 – Today, vagus nerve stimulation is usually used in conjunction with other medications and treatments.36 The pulse generator is about the size of a deck of cards and, like other neuromodulation devices, is used only when other forms of treatment don’t work.36
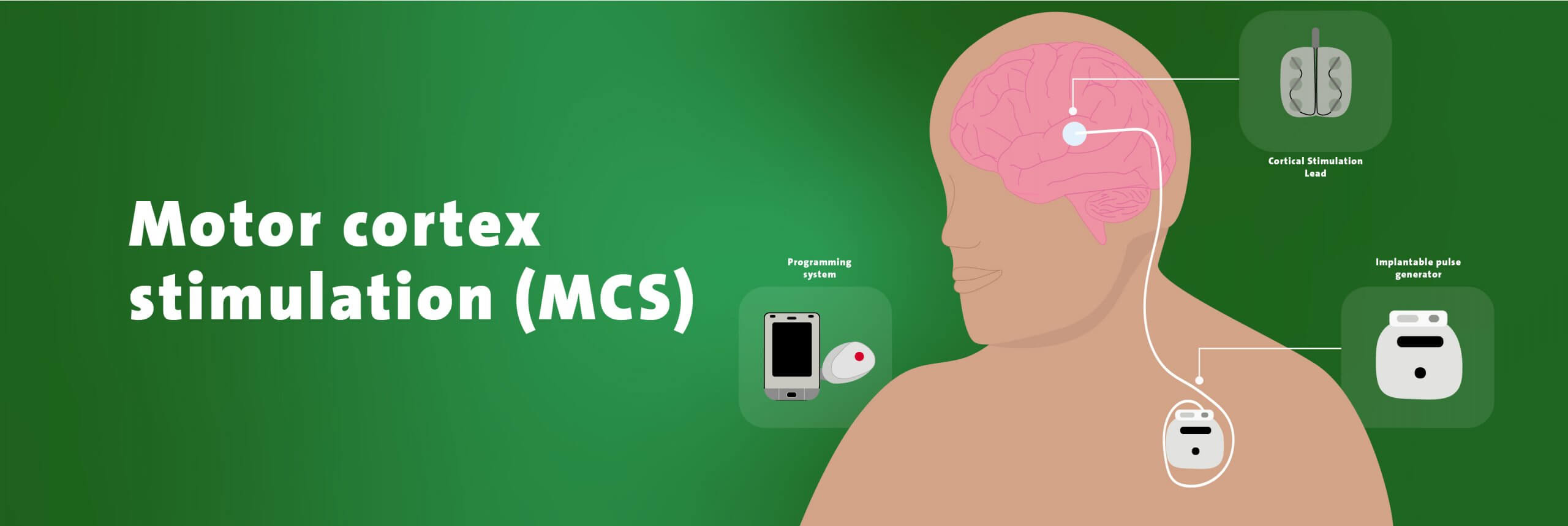
Motor cortex stimulation (MCS) is a last-resort treatment for chronic neuropathic pain. It features an implantable pulse generator to treat various pain syndromes and to rehabilitate patients after stroke.39 According to ReShape Lifesciences, 84% of patients experienced at least a 40% improvement in pain with MCS.38
Once you’re approved to get MCS, your doctor will order an MRI to pinpoint the area of your brain that will get stimulated. On the day of surgery, your surgeon will anaesthetize you before performing a craniotomy (removal of part of the skull), to implant the electrodes.42 Your surgeon may wake you during the procedure to test and adjust the device.
The device is about the same size as a pacemaker or an ICD and its pulse generator is usually placed in the chest wall.42
1991 – Tsubokawa and colleagues presented motor cortex stimulation (MCS) as an effective treatment for thalamic pain syndrome – a syndrome that usually occurs after a stroke, affecting the thalamus (a region in the brain).39,40 MCS was shown to provide long-term analgesia (inability to feel pain) in half of the patients who were resistant to medication.
2003 – In the Netherlands, MCS was observed in patients who suffered from chronic neuropathic pain as a part of an observational study. The study observed a decrease in pain scores, improved quality of life and a decreased consumption of pain medication.41
2017 – In South Korea, a study by Dr Cha, Um, Kwon, et al indicated that while MCS is a potentially effective treatment for neuropathic pain, repetitive stimulation could reinforce the modulation circuits of pain outside of the brain and spine, increasing the neuropathic pain threshold and withdrawal threshold of MCS.42
2018 – 700 patients have been treated with MCS worldwide.39
2020 – MCS has become more accessible over the years, but it’s only considered if other therapies and medications are proven to be ineffective in treating your pain symptoms.43 Consult your doctor to find out more about whether you’d be a candidate for MCS.
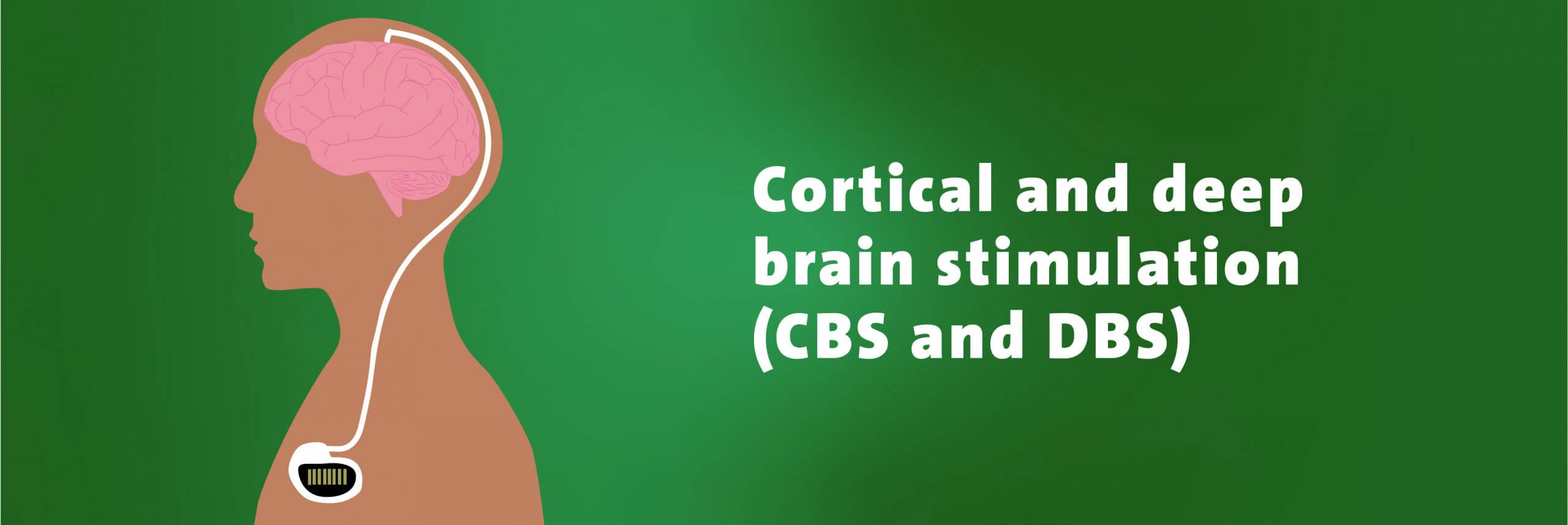
Cortical brain stimulation (CBS) is used for psychiatric diseases, obsessive-compulsive disorder, depression and minimally conscious state.43 The stimulation devices sends electric pulses to the surface of the brain. This pulse is delivered through electrodes powered by a generator and battery located in the chest.43
Deep brain stimulation (DBS) is used to treat Parkinson’s disease, epilepsy, dyskinesia (which can include muscle twitches), and symptoms related to stroke.43 In recent times, the use of DBS has extended to a variety of new diseases, such as refractive depression, OCD, obesity, eating disorders and drug-resistant hypertension.43
This type of stimulation is also delivered through electrodes from a pacemaker-like device, which is powered by a generator and battery located in the chest. The primary goal of DBS is to rebalance the damaged neuronal circuits by electrically manipulating certain brain structures.43
The implantation procedure is similar to MCS implantation in that candidates may undergo trial stimulation before having the device permanently implanted with a craniotomy.43 The implantation method involves an invasive surgery where microelectrodes are implanted into selective lesions of specific deep brain structures.43
1804 – Giovanni Aldini first experimented with electrically stimulating the human cerebral cortex on decapitated prisoners. Such experiments led him to conclude that stimulating the cortical surface could have therapeutic effects and therefore treat some neuropsychiatric disorders.43
1809 – Luigi Rolando electrically stimulated the cortex of animals.43
1870 – Gustav Fritsch and Eduard Hitzing were able to induce muscle contractions in dogs while electrically stimulating their cortexes.43
1874 – Robert Bartholow (American physician) electrically stimulated the cortex of an awake human for the first time.43
1882 – Ezio Sciamanna (Italian neuropsychiatrist) performed a series of experiments on a trepanned (hole in the skull) patient who had traumatic brain injury.43
1883 – Alberto Alberti (Italo-Argentine surgeon) conducted cerebral-stimulation experiments on a woman, which lasted eight months.43
1938 – Ugo Cerletti introduced electro-shock therapy to treat severe psychosis.43
1950 – Brain stimulation for pain control was first used by temporarily implanting electrodes into the brain.43
Late 1960s – The introduction of L-Dopa, medication for Parkinson’s disease, caused a sharp decline in surgical treatment.43
1962 – Melzach and Wall first developed the ‘gate control theory’ with data from brain stimulation for pain control. These experiments and theories led to the development of cortical brain stimulation and deep brain stimulation.43
Many doctors used a minimally invasive method of surgery to deliver deep brain stimulation. This method led to the discovery that low-frequency stimulation enhanced tremors and other symptoms, while high-frequency stimulation helped reduce symptoms.43
1963 – Natalie Petrovna Bekthereva, a neuroscientist from Russia, was the first to use deep brain stimulation to treat motor disorders. Bekthereva published her work on using multiple electrodes implanted in the brain to treat hyperkinetic disorders.43
Hyperkinetic disorder yields greater impairment and more impulse difficulties than attention deficit hyperactivity disorder (ADHD).43
Carl Wilhelm Sem-Johnson used depth electrodes to help treat patients with epilepsy and psychiatric disorders. He eventually found the most effective site for the treatment of Parkinson’s disease.43
The implants were left in the patient for many months without any adverse side effects.43
1970s – DBS was also used to treat chronic pain.43
1991 – Alim Louis Benabid (neurosurgeon, France), van Laere M Blonde (neurosurgeon, France), Jean Siegfried (neurosurgeon, Switzerland) and their respective teams reported that thalamic DBS – stimulation on the thalamus, which is a region in the brain – was effective for tremors.44
2020 – As the name suggests, deep brain stimulation is an invasive procedure that places electrodes deep into the brain.
Today, the device is just smaller than a deck of cards. The correct placement of leads and electrodes is usually guided by magnetic resonance imaging (MRI) or computed topography (CT) imaging.43
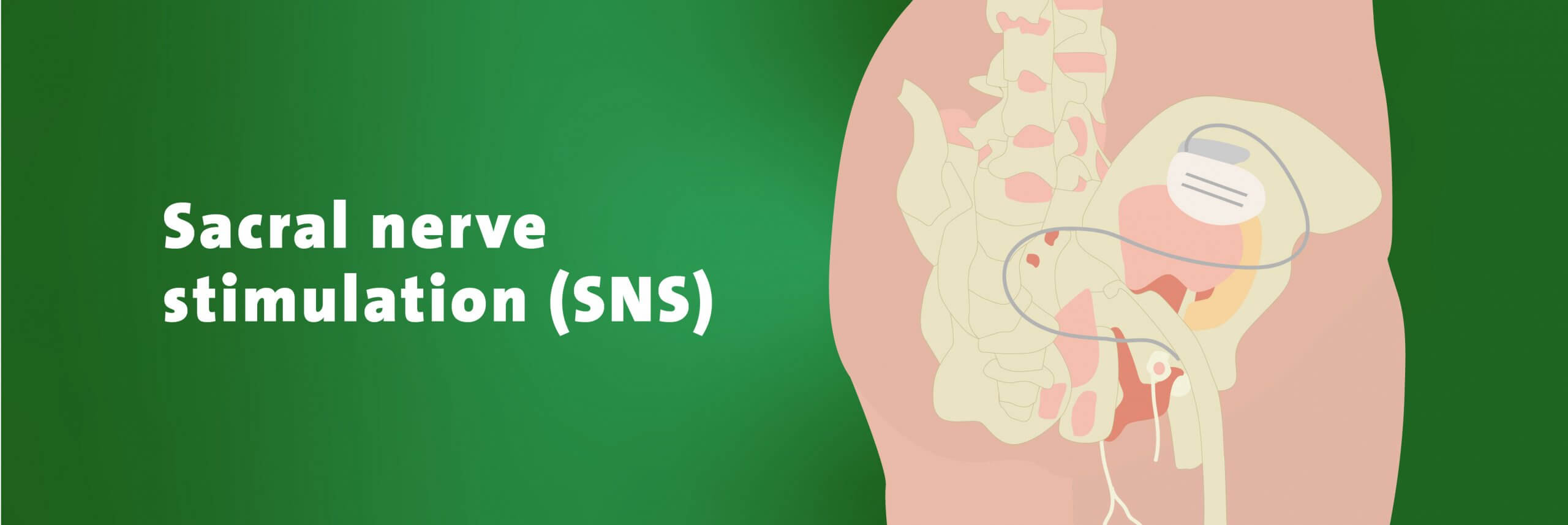
A sacral nerve stimulator (SNS) is an implantable device that’s used for intersim therapy. Intersim therapy involves using SNS to stimulate the sacral nerves, which controls a person’s bladder, bowel and pelvic floor muscles.44 Interstim therapy has never been withdrawn from any country.45
The implantation procedure is carried out in two stages. In the trial stage, the surgeon will create a small incision in the buttock with x-ray assistance. The leads are guided through a small hole in the sacrum called the ‘third sacral foramen’ along the path of the third sacral nerve.47 In stage two, if the patient experiences a significant improvement, the surgeon will remove the external lead and insert a pulse generator. The pulse generator is usually placed just above the hip bone.46
1981 – Sacral nerve stimulation was first introduced by Tanagho and Schmidt to treat urinary urge incontinence.44
1991 – The FDA approved SNS for urinary urge incontinence.45
1994 – Medtronic received the CE mark for Interstim therapy for chronic intractable pelvic and lower urinary or intestinal tract disorders. Interstim therapy was also approved for use in Australia and Canada.46
1997 – Interstim therapy was approved for use in the US for urinary urge incontinence.45
1999 – Interstim therapy was also approved to treat urinary urgency, frequency and retention.44
2006 – A study by Wallace et al. discovered the effectiveness of SNS in treating a range of underlying neurologic diseases, such as multiple sclerosis, Parkinson disease, spina bifida and spinal cord disease.44
2020 – Today, current pulse generators are just smaller than a deck of cards and can last up to five years. A surgeon can remove the old pulse generator and replace it with a new one as needed. Rechargeable pulse generators, which can last over 10 years, may become available soon.46
Humans have come a long way since 1804 when Giovanni experimented with electricity on decapitated prisoners.29 The current global medical implant market is worth an estimated USD$112billion, with a compound annual growth rate of 7.07% for the period 2017-2023.48
Even so, there is still great potential for growth in this ever-evolving field. With the emergence of new technologies, we hope to see many more life-changing medical innovations in the years to come.
Health insurance can help cover the costs of treatment for many medical conditions. Compare a variety of policies from insurers in Australia by using our free health insurance comparison service.
So, what are you waiting for? Compare health insurance today.